
A Complicated Case of the Heart – FDA Meets on Heart Safety of Diabetes Drugs
By Kelly Close
.jpg) Twitter summary: .@kellyclose testifies on patient perspectives on heart safety for #t2 #diabetes drugs
Twitter summary: .@kellyclose testifies on patient perspectives on heart safety for #t2 #diabetes drugs
The FDA just held a public meeting to discuss the results from two major heart safety trials conducted on the DPP-4 inhibitor drugs Onglyza and Nesina. Both trials suggested that the drugs do not increase the risk of cardiovascular events, such as heart attacks and strokes. Following a long day of testimonies, the FDA committee voted that both Onglyza and Nesina passed the heart safety requirements necessary to stay on the market. The committee further voted that both drugs should have their labels updated to reflect the findings from these important trials. But the day’s discussion was not just about drug labels – it brought up (at least for some) much bigger questions about where we are spending our research dollars, and how these heart safety trials are (and are not) actually impacting patients.
These heart studies, also called cardiovascular outcomes trials or CVOTs, became a mandatory part of the FDA drug approval process back in 2008. Following concerns that Avandia increased the risk of heart attacks (that were subsequently overturned), the FDA decided that all diabetes drugs should prove they are heart safe. But since cardiovascular events occur infrequently, companies must conduct multi-year, large, and expensive trials on people at high risk for cardiovascular events to demonstrate that their drugs are safe.
 I spoke to the FDA panel that day, because as a patient, I want a world where money is spent on the drugs that work. That means making sure money isn’t wasted on inessential medicines or clinical trials that aren’t providing clear benefits for patients. My full talking points can be found here, and my slides from the presentation can be found here.
I spoke to the FDA panel that day, because as a patient, I want a world where money is spent on the drugs that work. That means making sure money isn’t wasted on inessential medicines or clinical trials that aren’t providing clear benefits for patients. My full talking points can be found here, and my slides from the presentation can be found here.
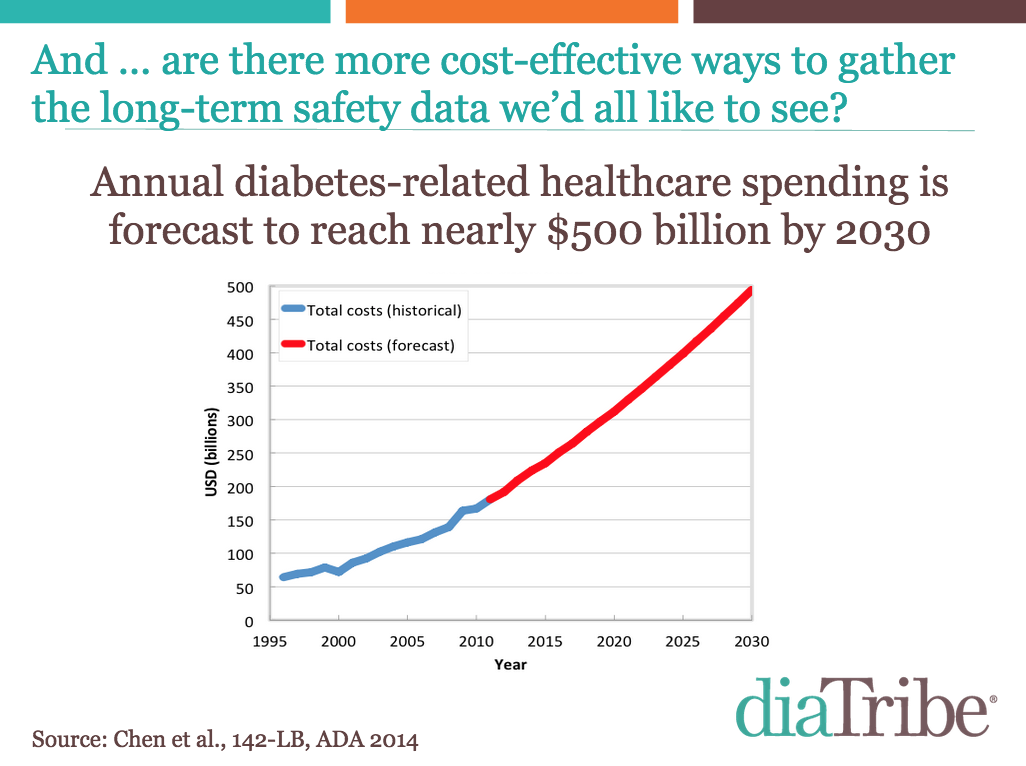
The two trials discussed, combined, cost $300 million dollars. When I hear that number, I think of all that we could do with $300 million. How many bottles of drugs could that supply? How many bottles of insulin? How much other research could we get with these resources? We’re only spending $50 million a year on diabetes prevention in the US – how many people could we prevent from getting type 2 diabetes with $300 million?
 If these trials gave definitive, clear outcomes on the effects these drugs have on heart health, that’d be one thing. But the unfortunate truth is that they aren’t. For numerous reasons, these trials were not designed in ways that give us this definitive, clear data we need. As I stated, “These two trials likely sunk $300 million, and we’re not really sure we have the right data!”
If these trials gave definitive, clear outcomes on the effects these drugs have on heart health, that’d be one thing. But the unfortunate truth is that they aren’t. For numerous reasons, these trials were not designed in ways that give us this definitive, clear data we need. As I stated, “These two trials likely sunk $300 million, and we’re not really sure we have the right data!”
The reality of these long, expensive trials has been disappointing, but both patients and the FDA can agree that we want the same thing – clearer results that can be used to improve treatment for diabetes. Before we spend another $300 million on these trials, let’s take what we’ve learned, coordinate, and design safety trials that better benefit the patient community.
very best,

Kelly Close
To read more background on CVOT trials, please see my previous article here.






