
Does This Insulin Make Me Look Fat?
By Julie Heverly
 Weight impacts diabetes and diabetes impacts weight. The emotional and physical toll of excess weight is not exclusive to the type 2 diabetes community as diaTribe staff member, Julie Heverly explores.
Weight impacts diabetes and diabetes impacts weight. The emotional and physical toll of excess weight is not exclusive to the type 2 diabetes community as diaTribe staff member, Julie Heverly explores.
Within a year of giving birth to my daughter, I accepted a new job and my husband and I left Philadelphia and relocated 350 miles west. I was excited to return to Pittsburgh, where I could raise my daughter closer to family and start a new adventure. Moving as a person with diabetes means finding all new members of your medical team including endocrinologists, diabetes educators, dietitians, ophthalmologists, podiatrists, primary care physicians, dentists, and a few other specialists.
Finding a new doctor you connect with is challenging; establishing an entirely new health care team is daunting. But I was on top of the world with my miracle baby, dream job, new house, and a decent A1C. I made my appointment with the largest endocrine practice in the city and headed to my first appointment.
At that point, I had been living with type 1 diabetes for 16 years. I had volunteered and worked for the American Diabetes Association all along the east coast in Maryland, Virginia, and Pennsylvania collectively for more than decade. I was spending my professional and free time fundraising to support research to prevent, cure and improve the lives of people who were affected by diabetes. And I had gone through a pregnancy which was high risk because of my diabetes and had been treated by a renowned endocrinologist on the East Coast.
But what happened at that first appointment will never leave me.
It ranks high on my list of the most insulting, frustrating and ill-informed conversations I have ever had with a medical professional. In fact, sharing it with you here many years later is still painful, but without question the conversation around type 1 diabetes and weight issues needs to happen.
The endo assigned to me that day began our appointment by asking, “How would you like to come off insulin?”
In shock and dismay, I responded, “As a type 1 AND the executive director of the American Diabetes Association here in Pittsburgh, I assure you that curing type 1 diabetes is one of my personal and professional missions. A cure will be the only way I can come off of insulin. Do you have a cure?”
And that’s when she said “it.” The words that I can still hear: “I’ve never seen a type 1 patient as…” (and there was an awkward pause) “… large as you. Type 1s are usually thin and diagnosed in childhood and you are neither. I think you might have been wrongfully diagnosed. Wouldn’t you like to know for certain?”
She babbled on about type 2 diabetes and people who are misdiagnosed after the age of 18. I can’t recall the entire conversation because my brain was reeling with facts that I felt she clearly did not know. My emotions were all over the map with confusion, embarrassment and the kind of anger caused by hurt that makes people do crazy things.
 I was in my mid- to late-30s. I had just had a baby. I was overweight, and yes, my BMI was considered obese, but not extremely or morbidly obese. Did I mention I had just had a baby? Did she care that I was diagnosed 16 years earlier and at the time was much thinner and a collegiate athlete?
I was in my mid- to late-30s. I had just had a baby. I was overweight, and yes, my BMI was considered obese, but not extremely or morbidly obese. Did I mention I had just had a baby? Did she care that I was diagnosed 16 years earlier and at the time was much thinner and a collegiate athlete?
Diabetes is shrouded in guilt, stigma, self-doubt, and a constant need to address our health questions, all the while feeling responsible for addressing cultural misunderstandings about diabetes. People with diabetes always have to educate and explain what we’re doing, why we’re doing it, and many times that yes, we can be doing it. I expect ill-informed questions from the woman in the restaurant, the kid on the bus, or the guy at work. I do not expect, or accept, those type of questions from a specialist in the field.
Sixteen years, 64 blood draws, C-peptide tests, two clinical trials, a high-risk pregnancy, and 5,840 days of managing my blood glucose with finger sticks, insulin and exercise – my type 1 diagnosis and need for life-sustaining insulin was never in doubt.
Insulin is a hormone that regulates blood glucose levels and aids life by converting carbohydrates into the body's primary source of energy. Without it, people with type 1 diabetes cannot process nutrients, cells start to malfunction, patients lose weight rapidly and eventually perish. In the single month leading up to my diagnosis, I dropped almost a pound per day. What I thought was the best diet ever, turned out to be organ failure. I was diagnosed with type 1 diabetes wearing a size 8.
Insulin keeps me alive and I am grateful to Dr. Frederick Banting and Charles Best for discovering a way in which insulin could be extracted and made available to people with diabetes to extend our lives. Have you ever seen the before and after pictures of one of the first children who received insulin 100 years ago? Take a look; the life it provided to him is amazing!
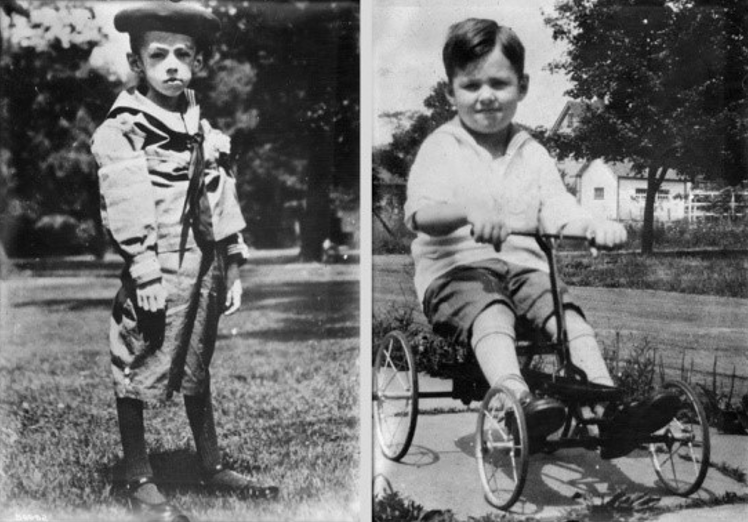 Do you see how emaciated he was pre-insulin? After receiving insulin, he looks healthy. Do you also notice that there is more “meat” on his bones after taking insulin?
Do you see how emaciated he was pre-insulin? After receiving insulin, he looks healthy. Do you also notice that there is more “meat” on his bones after taking insulin?
That is because insulin stimulates our muscle, fat, and liver cells to absorb glucose during digestion and that glucose can either be used for energy or converted and stored as fat. Having diabetes and needing to inject insulin can have dramatic effects on a person’s weight. An endo once explained that hypoglycemia can lead to someone eating excess carbs and calories, which then increases a person’s appetite, and body processes called the amylin effect (which causes you to feel full) as well as the incretin effect (which is when your body releases more insulin as a result of eating food with glucose in in) are diminished or absent in people with diabetes.
Since my dramatic weight loss at the time of my diagnosis, I have felt like I was in a Catch 22. Survival is a basic human instinct. Prioritizing health and a quality of life have been ingrained into me by my family. I required insulin to survive and to thrive, so I took it. But as soon as I started insulin therapy, the pounds I lost were immediately found (like the child pictured above) and added to my frame. I went from emaciated, to healthy, to overweight. The weight was a result of many misguided choices, as I tried to figure out how to navigate life with diabetes. Even knowing that, it still feels like the amount of insulin I take to live, is correlated to my weight – hence the title of this article – "Does this insulin make me look fat?"
In 2017-2018, the U.S. adult obesity rate was 42.4%, according to the Centers for Disease Control and Prevention (CDC). The CDC also states that type 1 diabetes can be diagnosed at any age and among all ethnicities and genders. Therefore, it’s fair to reason that someone who has type 1 diabetes MIGHT also be overweight or obese.
But why is it important to debunk these stereotypes that all people living with type 1 diabetes are thin and only people with type 2 diabetes have to think about weight management?
-
First, such generalities diminish all people with diabetes from living their best and healthiest lives. I’ve heard from others about equally upsetting comments from gynecologists, ophthalmologists, optometrists, dermatologists and primary care physicians who make false and stigmatizing comments and then recommend treatment based on such demonstrated bias and not on the person’s individual medical needs. Those comments have also caused the people with diabetes to delay or refuse treatment from the provider moving forward.
-
The assumption that all people with type 1 are skinny can lead to eating disorders like diabulimia, anorexia, or bulimia. According to the American Diabetes Association, “Eating disorders are probably more common among women with diabetes than women who do not have diabetes. Those with type 1 are twice as likely to suffer from disordered eating patterns. Bulimia is the most common eating disorder in women with type 1 diabetes. Among women with type 2 diabetes, binge eating is more common.” If you are concerned that you or someone else with diabetes may be experiencing disordered eating, contact the Diabulimia Helpline or We Are Diabetes; the National Eating Disorders Alliance is a resource for anyone with or without diabetes.
-
This assumption also makes it more difficult for people with diabetes to receive the proper care they need to successfully manage their weight and diabetes – which are often intertwined.
-
Finally, by recognizing that for some people with type 1 and people with type 2 there is a connection between insulin and weight gain, it would provide an opportunity for health care providers to treat the whole person in new, more effective ways. It could also encourage more clinical research to be conducted on the subject and eventually have new treatments to be developed, tested, and approved.
My confrontation in 2014 with that endo resulted in three follow-up phone calls because I felt that she needed to understand that her assumptions, stigma-loaded comments, and poor bedside manner needed to be corrected. I also spoke with her boss. Then I found a new endo. Her comments did not lead to a new diagnosis, nor did they end my insulin therapy, nor did they encourage me to lose weight. Sadly, over the next seven years I would continue to add weight to my middle-aged frame.
Weight impacts diabetes and diabetes impacts weight.
 I have spoken with fellow people with diabetes who have unsuccessfully tried nutrition plans, exercise programs, therapy, or even weight loss surgery. The frustration is palpable among them. One friend shared the frustration of working out, then experiencing exercise induced lows that required consuming even more calories than were burned just to bring their glucose levels back into range. Another friend shared that she is “living in fear of her own body,” worried about her type 1 diabetes, her weight and all the complications connected to both.
I have spoken with fellow people with diabetes who have unsuccessfully tried nutrition plans, exercise programs, therapy, or even weight loss surgery. The frustration is palpable among them. One friend shared the frustration of working out, then experiencing exercise induced lows that required consuming even more calories than were burned just to bring their glucose levels back into range. Another friend shared that she is “living in fear of her own body,” worried about her type 1 diabetes, her weight and all the complications connected to both.
They all seemed to feel that their diabetes has impacted their ability to have a “healthy relationship with food.” Health, weight, and diabetes management seem as volatile as blood glucose levels after eating pizza.
In the midst of the COVID pandemic, as I worked to educate people about the risk of COVID-19 to people with diabetes and co-morbidities, fear took hold of me. I began to frantically seek solutions that would work for me, not necessarily other 40-year old’s, or others with diabetes, but specifically for me.
Previously when I was upset about my weight, I would ask my endo for advice. They would have me meet with a dietician who would encourage me to measure my food and limit my carbs to no more than 45 carbs per meal. There was never a prescriptive plan. I still had to figure it out and I continued to guess wrong. I would eat 45 carbs per meal, but it would not sustain me for very long and I used to be hungry all the time. Between meals I would supplement my diet with no or low carb options, such as cheese, avocado, protein, and nuts.
About six years ago, I specifically discussed these high fat, low carb foods supplementing my diet with my healthcare team and was encouraged NOT to take them out of my diet for fear that it would lead to me eating more carbs, therefore increasing my insulin intake or blood glucose levels.
However, I continued to wonder which was the bigger problem? Managing my blood glucose or the weight that impacted my diabetes?
I did not want to start something without my healthcare team’s input or blessings. I brought each and every idea to my endo and my primary care physician. They graciously allowed me to try some new options and worked with me through the entire process. Finally, I found a formula that worked.
In November 2020 I started taking a GLP-1 receptor agonist (off-label) and signed up for WW (formerly Weight Watchers). For years I had been trying one thing at a time to see how it would work. But I knew if I wanted different outcomes, I needed to try a different method. So this time I tried multiple things at once.
The Food Journey: Over the years I’ve tried many diets with varying degrees of success. For me, the challenge with diabetes and nutrition is that food is both venom and antidote – needed for survival but also capable of killing you. After doing some research and talking with my care team and some friends with diabetes, I decided to try WW.
WW personalizes a plan based on your age, weight, height, and gender and then provides a daily points allotment to guide your food choices. Every food has a points value based on its nutritional content, with fresh fruits and vegetables having no points at all. It’s calorie counting simplified, something I found particularly helpful since I was still having to count carbs for medicating. A dual tracking approach to food can be complicated, but over time and with practice it became much easier. Tracking all my food also provided perspective about the low carb foods that I had been eating in abundance. I quickly realized 90% of them would have to go. They would become treats, not staples.
While I was learning this new way of approaching food – the GLP-1 receptor agonist I was using was helping to curb my appetite and more effectively utilize the insulin I was taking. My decreased appetite was tremendously helpful in keeping me within the daily WW points. In my first seven weeks, I lost 19 pounds and had successfully made it through the Thanksgiving and Christmas holidays feeling better, lighter, and more proactive.
The Exercise Journey: In January, I joined Diabetes Strong’s “Fit with Diabetes Challenge.” I had been walking throughout the first nine months of the pandemic, but I was missing my Pilates sessions since my gym was closed. It was a six-week program that I hoped would keep me accountable as I worked on reintroducing exercise into my routine. I was encouraged to set a goal of exercising 20-30 minutes 4-5 times a week for the first six weeks of the year. The challenge also provided information about dealing with diabetes while working out which has always been a very tricky issue for me.
Throughout all of this, I regularly checked in with my health care team. The dramatic alterations in my diet, the addition of exercise, and my use of a GLP-1 meant constantly adjusting my basal rates as well as my carb ratios. I am now ten months in and I still track all of my food and beverages in the WW app, exercise five to six days a week, take my GLP-1 weekly – as a result, I have reduced my insulin intake by almost half. Each of these factors has been one part of the winning combination that has helped me to lose more than 70 pounds, get and keep my A1C under 7%, and my Time in Range around 70% for almost a year!
 It has taken many trials and failures to get where I currently am and my journey is far from over. I know this is as fragile an ecosystem as keeping my blood glucose levels in the correct range. I delight in my new-found health, energy and clothing size (not an 8 again yet, but much healthier). But I also worry about maintaining this formula. I worry that if my schedule shifts, it could become more difficult to find time to exercise and prepare healthy meals. Diabetes is a progressive illness and over time, my body could naturally require more insulin or develop new insulin resistance. My GLP-1 could cease to be covered by insurance and since I’m using it off-label it could also no longer be affordable for me. I worry about all of those things, a lot.
It has taken many trials and failures to get where I currently am and my journey is far from over. I know this is as fragile an ecosystem as keeping my blood glucose levels in the correct range. I delight in my new-found health, energy and clothing size (not an 8 again yet, but much healthier). But I also worry about maintaining this formula. I worry that if my schedule shifts, it could become more difficult to find time to exercise and prepare healthy meals. Diabetes is a progressive illness and over time, my body could naturally require more insulin or develop new insulin resistance. My GLP-1 could cease to be covered by insurance and since I’m using it off-label it could also no longer be affordable for me. I worry about all of those things, a lot.
This is my journey. Many of the other people I spoke with who have type 1 and are struggling with their weight have not experienced the same outcomes as me. The science experiments associated with diabetes management, exercise, and weight loss are like a house of cards. Each building block is dependent on the one next to it and can’t provide results alone. One change could be catastrophic and bring the whole thing down. It may vary daily throughout my life and it will always be something I have to fight to manage and maintain. But diabetes has taught me that health stability is something worth fighting for and working towards.
Want to learn more about obesity and weight management? Register for diaTribe's 8th Annual Solvable Problems in Diabetes panel happening on September 28 at 9:30 am PDT / 12:30 pm EDT / 17:30 BST / 18:30 CEST! Click here to learn more and sign up.







