
How Race and Ethnicity Affect Diabetes Prevalence, Management, and Complications
By Julia KenneyMatthew GarzaEliza Skoler
Black, Indigenous, Hispanic, and Asian individuals, and people of all non-white racial and ethnic groups are more likely to have diabetes and diabetes-related health complications than their white peers. Here’s how social determinants of health lead to differences in diabetes care and outcomes, creating racial, ethnic, and economic health disparities in the United States.
According to the 2020 National Diabetes Statistics Report published by the Centers for Disease Control (CDC), diabetes affects over 34 million people in the United States – that’s more than one in ten people. However, diabetes does not affect all communities equally. As with many conditions – such as heart disease, chronic lung disease, and chronic kidney disease – a person’s race, ethnicity, and socioeconomic status influences both their risk for developing diabetes and their access to diabetes management resources. The health disparities that exist among the many races in the US are not attributable to genetics or biology alone, but also to socioeconomic factors and social determinants of health that disadvantage people of color.
Though genetics and biology do play important roles in diabetes prevalence and complication rates, this article will focus on the societal factors that affect the lives of people living with diabetes – such as access to healthy food, healthcare, employment, and other socioeconomic factors. We aim to specifically explore the racial health disparities that disadvantage communities of color. We will also highlight some of the factors underlying the concerning patterns in diabetes prevalence, management, and complications, and share ways to promote health and access to care for people with diabetes, regardless of race and ethnicity.
Defining Key Terms
-
Race & Ethnicity – Race is a socially constructed way to group individuals based on skin color and physical features. There is no specific set of genes that defines a race. Ethnicity is also socially constructed, and it categorizes people based on a shared sense of group membership (like language, culture, history, or geography).
-
Socioeconomic status – Socioeconomic status is a measure of a person’s economic and social standing. This term is often used interchangeably with social or economic class.
-
Health disparities – Health disparities are differences in health outcomes among various populations or communities. They are closely linked to social, economic, and environmental disadvantages that affect groups that have systematically experienced greater obstacles to health (due to factors including race, gender, age, sexual orientation, and economic status.)
-
Health equity – Health equity is the goal that every person, regardless of their background or circumstance, is able to live a healthy life with full access to quality healthcare and other health resources. Achievement of health equity requires valuing every person equally and addressing avoidable inequalities with focused, societal efforts to eliminate injustices and health disparities.
-
Social determinants of health – These are factors that influence a person’s health but fall outside the scope of a healthcare professional’s influence. They are the conditions in which people are born, grow, live, work, and age. For example, social determinants of health can include a person’s race, gender, socioeconomic status, education, and where they live and work; these factors are often longstanding and have multi-generational effects. Social determinants of health are one of the major causes of health inequities – the unfair and avoidable differences in health status.
-
Systemic racism – Also called institutional or structural racism, it is defined by systems and structures (such as medicine or the healthcare system) that have procedures or processes that disadvantage people of color.
Systemic racism lies at the center of this article. As we discuss racial health disparities and their underlying causes, keep in mind that these factors are a result of the long-standing structures that affect the lived experiences of people of color – they are not attributed to the personal decisions of individuals.
A Look at Racial Health Disparities in Diabetes
What do health disparities actually look like in the US? The data show concerning patterns: Black, Indigenous, Hispanic, and Asian populations are more heavily affected by diabetes than their non-Hispanic, white counterparts, in diagnoses, management challenges, and diabetes-related complications.
The CDC’s diabetes statistics report showed alarming differences among races in the estimated percentage of adults with diabetes (both diagnosed and undiagnosed) in the US from 2013 to 2016:
-
Black, non-Hispanic: 16.4%
-
Asian, non-Hispanic: 14.9%
-
Hispanic: 14.7%
-
White, non-Hispanic: 11.9%
While these differences in rates are stark, the evidence shows that diabetes prevalence is not dependent on race from a genetic or physiological standpoint alone. For example, in this study from 2007, when researchers accounted for socioeconomic factors, the differences in rates of type 2 diabetes between racial groups were reduced. This supports the idea that socioeconomic factors that disadvantage people of color are a significant cause for these health disparities.
In a 2017 study published in the Journal of Racial and Ethnic Health Disparities, a team of researchers from Meharry Medical College and Vanderbilt University found that there were differences in the quality of diabetes care between racial and ethnic groups. Using the 2013 Medical Expenditure Panel Survey (MEPS) data, they looked at adherence to five ADA-recommended services over one year that indicate quality of diabetes care. Compared to white individuals, Hispanic, Black, and Asian individuals received fewer diabetes management checks, including A1C tests, eye exams, foot exams, blood cholesterol tests, and flu vaccines. Even in adjusted models which controlled for factors like insurance coverage, poverty, and education, some of the disparities remained. Most notably, Hispanic, Black, and Asian individuals were still less likely to receive the two recommended annual A1C checks. The researchers showed that this difference in quality of care occurred partly because populations of color had less access to health insurance and diabetes management education, compared to white populations.
Trends in care translate to trends in diabetes outcomes – including complications and death rates. A study from 2014 looked into racial and ethnic differences in diabetes complications and mortality. Black, Indigenous, and Hispanic individuals had higher rates of retinopathy, end-stage kidney disease, and amputations than non-Hispanic white individuals. Furthermore, these groups were more likely to die from diabetes than non-Hispanic white Americans:
-
Indigenous populations were 3 times more likely to die from diabetes
-
Non-Hispanic Black Americans were 2.3 times more likely to die from diabetes
-
Hispanic Americans were 1.5 times more likely to die from diabetes
Just as with the risk of diabetes, people of color are not genetically predisposed to diabetes-related complications due to race alone. A combination of social and environmental factors plays into a person’s ability to successfully manage their diabetes.
How Genetics and Biology Are Involved
Racial and ethnic categories are not as closely associated with genetics and biology as some people think. In fact, categories such as white, Black, Asian, and Hispanic are defined more by society than by any set of specific genes. However, to fully address the factors that affect diabetes prevalence and outcomes, we must understand the role of genetics and biology. Studies have shown that there are biological differences among races that correspond to how a person metabolizes (or utilizes) glucose, their insulin sensitivity, and how fat is distributed in the body – however, a person’s family history of diabetes is more telling of their genetic risk for that condition than the color of their skin. The research on how genetics, biology, and race all intersect and interact to influence diabetes is complex; there is still much to determine.
As discussed, genetics alone do not explain diabetes-related health disparities among the races. Furthermore, we cannot reduce the large health disparities by focusing solely on biological factors, which are largely predetermined; we must instead focus on the socioeconomic factors and social determinants of health that exacerbate racial disparities, which are in large part founded in longstanding systemic racism. Below we describe some of the many elements of systemic racism that affect a person’s ability to manage their diabetes and receive quality diabetes healthcare.
Main Causes of Racial Health Disparities in Diabetes Prevalence
The factors we discuss here are influenced by systemic racism that is built into the social, economic, and political fabric of the United States. The systemic racism that people of color experience results in things like lower wages, fewer academic and professional opportunities, and reduced community resources. With this in mind, factors like income, unemployment, health insurance, and food and exercise environments are not entirely personal choices, but can be explained by a number of external causes.
Income
In the US, there are major racial differences in wealth. A 2018 Kaiser study offered this breakdown of people living below the federal poverty level:
-
1 in 4 Indigenous people
-
1 in 5 Black people
-
1 in 5 Hispanic people
-
1 in 10 white people
Further statistics on income and poverty levels can be found in the US Census Bureau’s 2019 report, which confirms the racial disparities in poverty rates. People living with incomes below the federal poverty level in 2018 were earning only $12,000 a year (or $25,000 for a family of four). These families – and many above the federal poverty level – often can’t afford the nutritious food, safe exercise opportunities, and healthcare needed to prevent and manage diabetes.
Unemployment and Health Insurance
People of color in America are also more likely to be unemployed. According to the US Bureau of Labor Statistics, the rates of unemployment in 2019, broken down by race, were:
-
6.6% of Indigenous people
-
6.1% of Black people
-
3.9% of Latino and/or Hispanic people
-
3.1% of white people
These unemployment rates and racial disparities have been further exacerbated by the COVID-19 pandemic, which dramatically increased unemployment rates in the US. Though unemployment is closely tied to income, it can also influence a person’s access to health insurance, since many people receive health insurance from an employer.
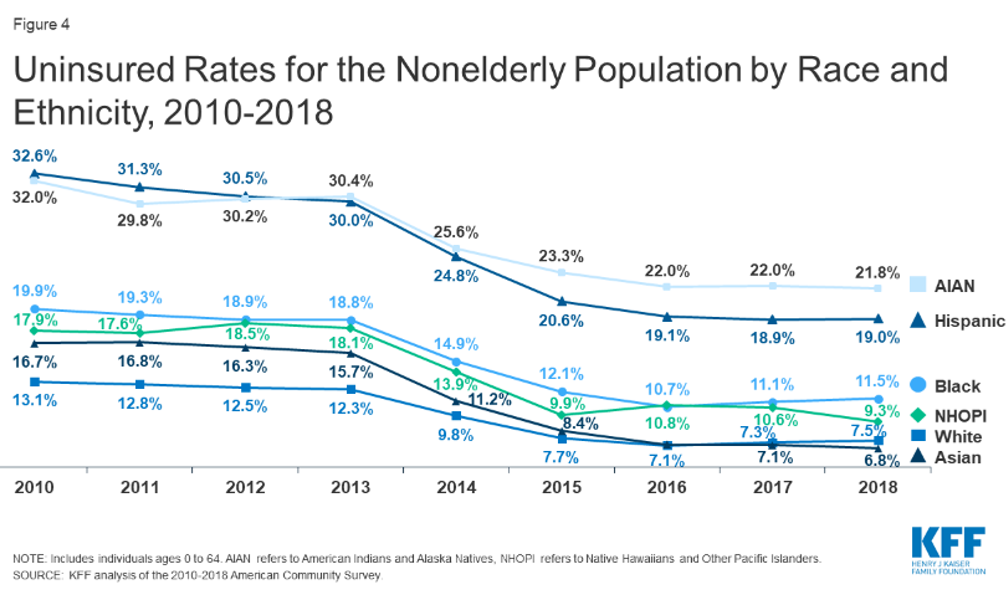 The high cost of healthcare means those who are uninsured or underinsured often do not get the care they need, including preventive healthcare (such as annual check-ups and prediabetes screenings) and instead must rely on inconsistent care. Unfortunately, Black, Indigenous, and Hispanic people are less likely to be insured in America. According to a Kaiser study of non-elderly individuals in the US, these were the rates of uninsured people in 2018:
The high cost of healthcare means those who are uninsured or underinsured often do not get the care they need, including preventive healthcare (such as annual check-ups and prediabetes screenings) and instead must rely on inconsistent care. Unfortunately, Black, Indigenous, and Hispanic people are less likely to be insured in America. According to a Kaiser study of non-elderly individuals in the US, these were the rates of uninsured people in 2018:
-
21.8% of Indigenous people (identified as American Indian or Alaskan Native
-
19% of Hispanic people
-
11.5% of Black people
-
7.5% of white people
Food and Exercise
A healthy diet and regular exercise are known to reduce the risk and improve the outcomes of type 2 diabetes. However, Black, Hispanic, and Indigenous communities in the US have less access to healthy foods and experience higher rates of food insecurity than white communities. According to the USDA, more than 35 million people lived in food insecure households in the US in 2019, including:
-
19.1% of non-Hispanic, Black households
-
15.6% of Hispanic households
-
7.9% of non-Hispanic, white households
Food insecurity is most common among low-income communities, which are disproportionately occupied by people of color. Moreover, food deserts (where there is little to no access to healthy foods) and food swamps (full of unhealthy fast-food options) are located primarily in minority neighborhoods. These communities are often faced with local food options that put them at an increased risk for diabetes: more small grocery stores with limited choices, fast food restaurants, and liquor stores, and fewer supermarkets with fresh fruit and vegetable options, bakeries, and natural and whole foods.
In addition to less access to healthy and affordable food, people of color often also have less time, money, and overall access to venues for exercise. This article from the New York Times about the racially exclusive culture around jogging is an eye-opening example of the barriers to exercise that many Black people face. Even at a time when some of the world’s most elite runners are African or Black, Black runners and joggers (in America, especially) often engage in protective measures such as running only during the daytime, steering clear of certain neighborhoods, or wearing Ivy League sweatshirts to deflect any suspicions that could lead to racist attacks.
Main Causes of Racial Health Disparities in Diabetes-Related Health Complications
Barriers to healthcare (such as a lack of health insurance or insufficient income) continue after a person is diagnosed with diabetes. Without ongoing, regular diabetes care, people face higher rates of health complications. Here are some of the barriers:
-
The high cost of insulin has made the life-saving drug inaccessible to many people, including people of color who have higher rates of unemployment and little or no health insurance. An American Action Forum report showed that insulin costs a person an average of $6,000 per year and found that one in four people with diabetes report rationing their insulin because they cannot afford the cost of their full prescribed dose.
-
Despite major advances in diabetes technology that make diabetes management easier, including wider use of CGM and insulin pumps, disparities exist in who has access to these tools. Black individuals are less likely to use an insulin pump or CGM than their white counterparts – which may be due to failure of the healthcare professional to write a prescription for technology, insufficient information about diabetes technology, an inability to afford these devices, or subtle racism on the part of the established medical system.
-
Even for people who have insurance, the costs of diabetes care and a diabetes-friendly nutrition plan can be challenging for people with low incomes.
Social and racial barriers widen diabetes health disparities. There is a history of prejudice against people of color in our healthcare system: Black, Indigenous, and Hispanic individuals can have the same income, insurance, and medical condition as white people yet still receive lower quality care due to systemic racism. In 2018, fewer than 12% of practicing physicians in the United States were Black, Hispanic, or Indigenous individuals. This means that there are fewer healthcare professionals who can earn trust and identify with communities of color. For more information on racism in healthcare, check out Unequal Treatment.
The Importance of Addressing Health Inequity in Communities of Color
It is clear that the disparities in diabetes prevalence, care, and management can be explained in part by of a number of social determinants of health, many of which are influenced by systemic racism. Every person with diabetes faces health barriers. But for many, the color of their skin can make successful diabetes management even more difficult and sometimes impossible. Every person with diabetes should have access to diabetes care, medication, and technology, and to living a healthy life with diabetes.
What Can We, as a Society, Do to Reduce These Disparities?
It will take extensive, collaborative, and creative work to address these disparities. We can begin by educating ourselves and others. Some good first steps include learning about the challenges faced by people of color with diabetes, about the people working to address these issues already, and about the ways to get involved. Check out some of our other articles on these subjects:
-
Health Equity: What It Means, Why We Care, and What You Can Do
-
Health Equity: A Framework for Improving Health Outcomes for People Living with Diabetes
-
Interview with Dr. Valerie Blue Bird Jernigan: Native Communities Working to Improve their Health
-
How Can We Make Mainstream Trends of Health and Wellness More Inclusive of Other Cultures?
-
American Diabetes Association Launches Campaign for Health Equity
-
Another excellent resource for learning and acting is diversityindiabetes.org
At diaTribe, we want to acknowledge the people and the organizations at the local, state, and national levels who are already doing the work needed to effectively tackle the health inequalities that lead to higher rates of diabetes and less favorable outcomes among people of color. In addition to those whose jobs focus on addressing health disparities, there are other ways for people to be involved in promoting health equity. Here are some ideas to consider:
-
Donate to national public health organizations focused on underserved communities. For example, the National Black Leadership Commission on Health, Inc., the Black Women’s Health Imperative, the National Alliance for Hispanic Health, and the National Indian Health Board.
-
Diabetes distress and the detrimental effects of dealing with systemic racism can both lead to poor mental health. Support organizations focused on overcoming the barriers to access and providing full mental health care to communities of color.
-
Find community health centers, multiservice organizations, food banks, and shelters in your city, county, and state – there might be a role for you as a volunteer or fundraiser.
-
Get involved politically; let your representatives at the local and national levels know how important it is to address health inequity.
-
Support policymakers in local, state, and federal elections who plan to address racial health disparities and have prioritized these issues in the past.
-
Join and support organizations like the ADA and JDRF that are leading health equity initiatives in research and advocacy for people with diabetes.
-
Continue to read diaTribe (subscribe to our weekly newsletter), as we continue to focus on health equity for all people with diabetes.
No matter what skills or resources you may have, determine how your expertise might be of benefit – particularly if you are in the health field where you can address systemic racism and health disparities. The more we learn about how the social determinants of health and racism in healthcare contribute to a person’s risk for diabetes and influence their diabetes management, the better prepared we’ll be to knock down barriers to quality care.
We acknowledge that every person should have the resources to manage their diabetes and, in the case of type 2 diabetes, to prevent it. All people, and especially people in positions of privilege, have a responsibility to help break down barriers to equal care for underserved communities. As people with diabetes and their allies, we have to do the work – and build upon the work already being done – to address racial health disparities and create more equitable and inclusive healthcare for people of color – in fact, for all of us.









