
Inhaled Insulin: Into Thin Air?
 by mark yarchoan
by mark yarchoan
Exubera never caught on, but several powerhouse companies are still betting on inhaled insulin. Does inhaled insulin have a future, or are other efforts bound to vaporize as well? At this point, all we know is that Exubera's was one of the costliest flops in the history of the pharmaceutical industry. Exubera had been in development for over 10 years, and its manufacturer (Pfizer) believed that it would be a very successful drug that would revolutionize the treatment of diabetes. However, in spite of high expectations and heavy promotion, Exubera failed to gain market traction - its sales amounted to less than one third of one percent of the insulin market. Pfizer pulled Exubera from the market in October, less than two years after the drug was first approved, citing poor sales and little faith in the products' future. The episode cost Pfizer $2.8 billion. What went wrong with Exubera?
exubera’s exuberance
Lack of simplicity wasn't Exubera's only problem. We also believe Pfizer underestimated the challenge of getting type 2 patients on insulin. "Insulin initiation," as they say is the business world, is just plain hard.
The bottom line, in our view, is that Pfizer was trying to introduce a consumer product that wasn't friendly to the consumer at all. It was just too complicated. We can point to the simplicity of Lantus, Januvia, and the OmniPod insulin pump as major advantages for these therapies/ technologies that are enjoying great levels of success Exubera didn't have this. Lack of simplicity wasn't Exubera's only problem. We also believe Pfizer underestimated the challenge of getting type 2 patients on insulin. "Insulin initiation," as they say in the business world, is just plain hard. National statistics show that over 60 percent of type 2 patients are not at A1c goal but only 29 percent of type 2 patients are on insulin. Ironically, insulin carries a stigma that deters many type 2 patients from its use, and many physicians are also not eager to introduce the therapy either because they are poorly reimbursed for their time and training or because they are pooly trained themselves and don't understand it well enough to help patients. A number of other factors contributed to Exubera's quick demise as well, in our view.
-
The inhaler was first-generation and imperfect - like many "first" generation medical devices. We don't think Pfizer should have advertised Exubera as "simple and trouble-free as an asthma inhaler" because the reality was far different. If a company isn't straightforward with patients, that's the first mistake! The inhaler resembled a bulky stapler, making it troublesome to carry around - perhaps if Pfizer had acknowledged this and discussed how it was working to make improvements, that would have helped (the next version would definitely have been better!). Pfizer also seems to have underestimated other elements, like difficulty in cleaning.
-
Long-term safety wasn’t yet established. Exubera caused a tiny decrease in the amount of that could be blown out in one second (FEV1), and also decreased some patient’s ability to pass oxygen from the lungs to the blood (DLCO). Although Exubera’s short-term safety was well documented (we had seen some eight-year data at EASD in Amsterdam last fall), and in most cases the breathing changes could be reversed when it was discontinued, long-term safety concerns about Exubera lingered. Moreover, patients were required to undergo lung-function testing both before using Exubera and after six months of use – this was also seen as “high hassle factor”. Sad to say, lung function testing presented an inconvenience to patients as well as to overworked physicians who sometimes didn’t even know where to advise patients to go for the tests, though the tests themselves only took 15 minutes or less.
-
Dosing was generally burdensome. Whereas injected insulin is traditionally prescribed in international units - no complicated conversion required - Exubera was prescribed in milligrams. A single milligram of Exubera was equivalent to about three units of insulin, but this relationship was not linear. For example, three milligrams of Exubera were equal to eight units of insulin rather than nine. That's confusing - and we think we're good at math!
-
Exubera was more expensive than injected insulin, and provided no benefits in efficacy. As a result, many insurance companies balked at paying for it. Almost every state's Medicare program as well as many private insurers placed Exubera in their most expensive tier. Exubera cost about $5 per day, compared to about $2-3 for insulin taken using a syringe and vial or a pen. Similarly, the National Health Service in the UK recommended against the use of Exubera because it had not been proven to be more effective than existing treatments. Germany also wouldn't pay for it.
-
The actual benefits were outweighed by drawbacks and were not broadly characterized as "breakthrough." For patients with "needle-phobia," Exubera did provide some relief from needles in administering rapid-acting insulins. Nevertheless, certain patients still needed to inject basal insulin in addition to taking Exubera. There really wasn't precedence for people to go on mealtime insulin before long-acting analogs - perhaps more studies should have been done on this front. Additionally, the needles for insulin have shrunk so significantly over the last decade that the burden of injections has decreased - as has the perception of the burden of diabetes! To most patients, the advantages of inhaled insulin did not outweigh the disadvantages. Furthermore, physicians felt encumbered in prescribing Exubera due to its complex dosing and lung function tests.
-
Pfizer didn't do a standout job marketing or selling Exubera. Although Pfizer developed Exubera with another company, Nektar Therapeutics, we didn't have the impression that Pfizer took full advantage of this collaboration - Nektar likely could have advised Pfizer better than anyone. In fact, Nektar, which received royalties from Exubera sales, was not even warned by Pfizer that the drug was going to be pulled from the market! Optimal communication between two parties is always difficult, but here it seemed particularly absent. We believe this would have helped Exubera succeed in the marketplace.
lessons learned and future directions
Pfizer was actually co-developing a second generation of inhaled insulin with Nektar called Next Generation Inhaled (NGI) insulin, but announced it would discontinue that effort as well. The inhaled insulin market is now completely open, and some manufacturers - MannKind, Novo Nordisk, and Eli Lilly (partnering with Alkermes) - continue to pursue their own inhaled insulins.
 MannKind is developing a product called Technosphere Insulin (TI). So far, over 3,000 patients have been treated with TI, and MannKind plans to launch this by late 2009 or 2010. Since Exubera's demise, MannKind has made notable attempts to differentiate TI, arguing that it will offer clinical advantages over vial insulin. Whereas Exubera peaked about an hour after administration and was therefore no more rapid than other available rapid-acting insulins, MannKind claims that TI will be absorbed in the blood stream almost instantaneously and will peak in only 12-14 minutes - much faster than other available rapid-acting insulins. This, the company says, will help to normalize post-prandial glucose levels and will lower the risk of hypoglycemia. We could all use less hypoglycemia, that's for sure. If MannKind can deliver on the promise, this should be positive for patients.
MannKind is developing a product called Technosphere Insulin (TI). So far, over 3,000 patients have been treated with TI, and MannKind plans to launch this by late 2009 or 2010. Since Exubera's demise, MannKind has made notable attempts to differentiate TI, arguing that it will offer clinical advantages over vial insulin. Whereas Exubera peaked about an hour after administration and was therefore no more rapid than other available rapid-acting insulins, MannKind claims that TI will be absorbed in the blood stream almost instantaneously and will peak in only 12-14 minutes - much faster than other available rapid-acting insulins. This, the company says, will help to normalize post-prandial glucose levels and will lower the risk of hypoglycemia. We could all use less hypoglycemia, that's for sure. If MannKind can deliver on the promise, this should be positive for patients.
TI should also be simpler for patients to use than Exubera. MannKind has previously announced that TI insulin will be dosed in units (not in milligrams) - this should be easier! - and will be administered by a device that is "small, simple, low maintenance, and easy to use." Also importantly, the existing four clinical trials of TI have shown no decline in lung function. Long may that last! Although lung-function testing will most likely still be mandated for TI users, the lung "sparing" of TI may help to convince patients and physicians of its long-term safety.
We cannot stress enough that insulin initiation is hard enough with the fear of hypoglycemia, weight gain and healthcare provider reimbursement. We praise all efforts to develop new, more convenient, and safer insulin-delivery methods.
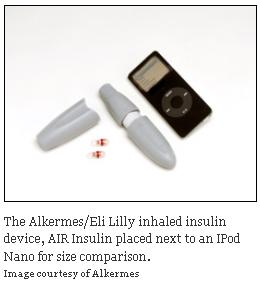
Alkermes and Eli Lilly and have teamed up to create an inhaled product called AIR Insulin. From what we've seen, their device is less than a fifth the size of the Exubera unit. We believe size and portability are very important.
Novo Nordisk’s inhaled insulin product, AERx IDMS is currently undergoing phase 3 studies. This device will use a single unit increment dosing system to deliver insulin. It is expected to come to market within the next few years.
These drug manufacturers know that many diabetes patients say that, all things being equal, they would rather receive insulin by inhalation than injection. Pfizer proved that inhaled insulin is possible and safe. Now, it's somebody else's turn to give us an inhaled insulin product that a good number of patients will want to use and that insurers will pay for at a reasonable rate. We cannot stress enough that insulin initiation is hard enough with the fear of hypoglycemia, weight gain and healthcare provider reimbursement. We praise all efforts to develop new, more convenient, and safer insulin-delivery methods.






