
Medications That Protect the Heart: New Data on SGLT-2s and GLP-1s
By Eliza Skoler
 By Joseph Bell, Eliza Skoler, and Rhea Teng
By Joseph Bell, Eliza Skoler, and Rhea Teng
Results from the VERTIS-CV trial show that SGLT-2 inhibitor Steglatro benefits heart and kidney health; hear expert opinions on SGLT-2 and GLP-1 medications
Dr. Samuel Dagogo-Jack and Dr. Christopher Cannon presented highly anticipated results from the VERTIS-CV trial, which studied the effects of Merck/Pfizer’s SGLT-2 inhibitor Steglatro (ertugliflozin) on over 8,000 participants with type 2 diabetes and cardiovascular disease (CVD). The trial found that treatment with Steglatro reduced average A1C by 0.5 percentage points, lowered average weight by nearly five pounds, and reduced blood pressure compared to standard diabetes treatment. Steglatro also improved kidney function, as measured by eGFR, and reduced the number of study participants with heart failure.
The researchers agreed that the VERTIS-CV results confirm the current guidance on the use of SGLT-2 inhibitors to prevent and treat heart failure and diabetes-related kidney disease. As a reminder, the current ADA Standards of Care advise using SGLT-2 inhibitors in people with type 2 diabetes for reducing hyperglycemia (high blood sugar), improving blood pressure, and facilitating weight loss. SGLT-2 inhibitors have also been shown to improve heart and kidney health in people with and without diabetes.
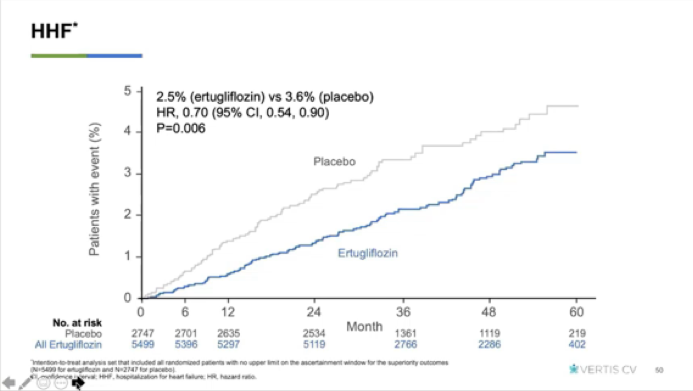
Compared to standard treatment, Steglatro did not significantly decrease the occurrence of major adverse cardiac events (MACE); this measurement takes into account the combined frequency of heart attack, stroke, and cardiovascular death. A different SGLT-2 inhibitor, Jardiance, has previously showed improvement in this category. Importantly, however, those taking Steglatro had a 30% lower risk of heart failure than did participants not taking Steglatro (see graph below). Even though it was not the “main point” of the trial, several healthcare professionals with whom we spoke found this result to be notable; it is a big deal for people at-risk for heart issues. Learn more about heart failure from our friends at the AHA.
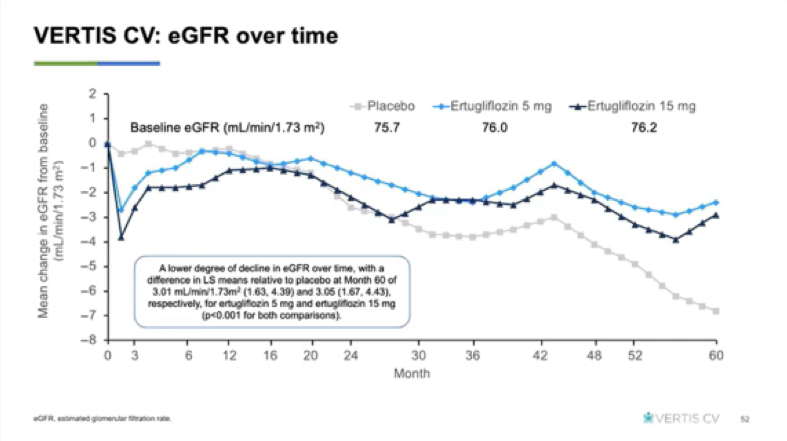
In terms of kidney disease, the graph below shows that those on placebo treatment experienced significantly more decline in kidney function than those on Steglatro.
Another presentation at ADA, by the Mayo Clinic’s Dr. Rozalina McCoy, showed who has access to therapies like SGLT-2s in the United States. Dr. McCoy highlighted the vastly lower use of DPP-4 inhibitors, GLP-1 agonists, and SGLT-2 inhibitors among people with type 2 diabetes on Medicare, compared to people with commercial insurance. Between 2013 and 2018, those on Medicare were:
-
39% less likely to be prescribed a DPP-4 inhibitor
-
55% less likely to be prescribed a GLP-1 agonist
-
69% less likely to be prescribed an SGLT-2 inhibitor
Given that these therapies are associated with lower weight and less hypoglycemia, we believe more people with diabetes should have access to them. While these medications are more expensive, we believe their advantages – reductions in heart failure and kidney problems – will save money in the long term.
Other important research emerged for people on GLP-1 drugs and at very high risk of heart failure, Harvard’s Dr. Elisabetta Patorno presented an intriguing real-world analysis of over 25,000 people with type 2 diabetes who added either an SGLT-2 inhibitor or a sulfonylurea to their GLP-1 treatment. The study found that the use of SGLT-2 inhibitor drugs significantly reduced negative heart health outcomes. Adding an SGLT-2 drug instead of a sulfonylurea was associated with a 24% decrease in a combination of heart disease incidents (myocardial infarction, stroke, and all-cause mortality) and a highly significant 35% decrease in hospitalization for heart failure.
We talked to some experts about this research.
-
Dr. Lawrence Leiter, University of Toronto: “As highlighted repeatedly in the presentation, there is nothing in the VERTIS [Steglatro] results that should change any guidance on the use of SGLT-2 inhibitors to reduce the risk of cardiovascular and renal disease. The challenge continues to be to get more of our patients on these (including GLP-1) evidence-based medications.”
-
Dr. Alice Cheng, University of Toronto: “I continue to agree with the recommendations from around the world on the use of SGLT2 inhibitors for cardiac and renal benefit, and the individual clinicians will need to make decisions with the person living with diabetes.”
-
Dr. Mikhail Kosiborod, Saint Luke’s, Kansas City, Missouri: “VERTIS-CV confirms that the two key benefits of SGLT-2 inhibitors – specifically, prevention of heart failure and favorable effects on preservation of kidney function – are class effects. I believe that when it comes to these two most common and morbid cardiovascular complications of type 2 diabetes (heart failure and diabetic kidney disease) – the benefits of SGLT-2 inhibitors are robust and consistent.”
-
Professor Philip Home, Newcastle upon Tyne, England: “To summarize: this class is not MACE protective, although there may be advantage to MI protection in some people; the class including Steglatro does prevent heart failure even in people with no prior CV disease. The same applies to declining renal function, perhaps the biggest clinical advantage of the class."
Everyone has different approaches to their diabetes management based on a number of factors, including risk of complications (like heart disease and kidney disease), hypoglycemia, weight, ease of use, and cost. diaTribe urges all people with diabetes to talk with their healthcare professional at least every six months to discuss their diabetes management, both in terms of glucose levels and preventing and treating complications.







