
Your A1C May Not Be Reliable If You Have Chronic Kidney Disease
By Matthew Garza
 By Matthew Garza
By Matthew Garza
Chronic kidney disease is a major complication associated with diabetes that can lead to inaccurate A1C measurements. Here we explain why this is and what you can do to manage your blood sugars if you have kidney disease
The high glucose levels that can be associated with many years of diabetes can lead to serious medical issues, referred to as diabetes complications. One is chronic kidney disease (CKD), also called diabetic kidney disease (DKD). As we have previously discussed, A1C is an important measurement used to assess overall diabetes management and risk for complications, but it does have multiple limitations. Since A1C is one value that reflects glucose levels over the preceding months, it does not show daily glucose trends or inform about hypoglycemia. When someone has chronic kidney disease, the ability to rely on their A1C value is compromised. This article addresses the limitations in A1C accuracy for people with CKD.
It is important to talk with your healthcare team about some of the challenges and limitations of A1C – read up on Beyond A1C here – so that you can understand that A1C is not the only accurate or reliable measure for monitoring your diabetes. You can discuss alternative measurements of diabetes management, such as time in range (TIR), with your healthcare team.
What is chronic kidney disease and how does it relate to diabetes?
The kidneys are important organs in our body responsible for a number of essential functions, including:
-
Removing waste products from the blood and other body fluids
-
Balancing the fluids and salts in the body
-
Helping manage blood pressure
-
Activating Vitamin D, which helps keep bones healthy
-
Helping make chemicals that stimulate the bone marrow to make red blood cells
When the kidneys are unable to function properly and filter the blood passing through them, that breakdown leads to CKD. The buildup of waste in the blood can lead to a variety of symptoms, from cramps to nausea and vomiting, to changes in your urine frequency and volume, or most commonly, in the early stages, no symptoms at all – which is why it is important to get your kidney health checked regularly. You can learn more about CKD and diabetes here, including the tests that healthcare professionals use to check your kidney function.
Diabetes and CKD are very closely linked. According to the National Kidney Foundation, diabetes is the leading cause of CKD. Chronic high blood sugar levels, and the high blood pressure that may be associated with the development and progression of CKD, can damage the kidney’s small blood vessel filtering system and contribute to kidney failure. Check out and download our infographic on diabetes and CKD here.
How does CKD affect A1C in people with diabetes?
Research shows that A1C, as a measure of blood sugar management, may be less accurate for people with CKD, especially those with advanced CKD (this means kidney function <60 mL/min/1.73 m2 or on dialysis). Declining kidney function decreases the reliability of A1C measurements leading to wide variation in the glucose/A1C relationship. This reflects that A1C measurements depend on both blood sugar levels and red blood cell production. In people with CKD, red blood cell production is lower for a number of reasons. This may lead to low red blood cell count (anemia), the need for blood transfusions, and the use of iron supplements or erythropoiesis-stimulating agents (medications that tell the bone marrow to make more red blood cells).
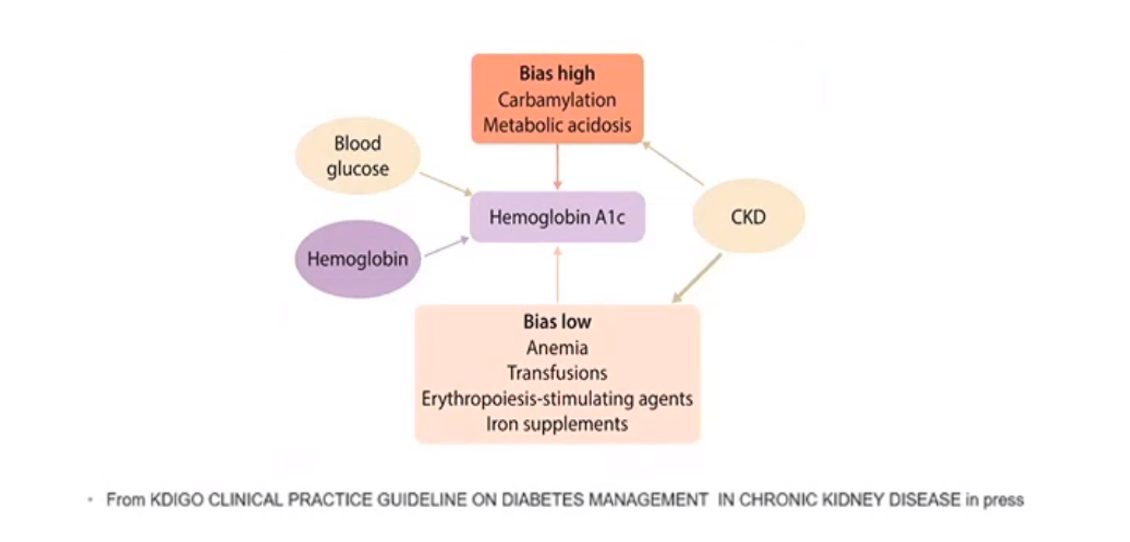
This graphic shows some of the reasons why CKD may overestimate or underestimate a person’s actual A1C. Some of the effects of having CKD can lead to an A1C that appears higher than it might actually be. For example, when the kidneys begin to fail, they are unable to remove acids that build up in the body (in the figure, this is called metabolic acidosis). The buildup of acid changes the proteins in your red blood cells (hemoglobin), causing a higher A1C even if you are not experiencing hyperglycemia. Another process that alters hemoglobin is carbamylation, which also produces a higher A1C, even when hyperglycemia does not occur.
On the other hand, CKD can also lead to an A1C that is seemingly lower than it actually is. CKD can result in reduced red blood cell production, leading to anemia (a lower-than-normal red blood cell count), or the need for blood transfusions or medications that help your body to make more replacement red blood cells. As a result, your A1C (which is affected by the amount of circulating red blood cells) may appear lower, or healthier, than it actually is. Therefore, it is critical if you have CKD that you discuss your A1C target with your healthcare team to find strategies that make sure you do not compromise your diabetes management – if you don’t already have a continuous glucose monitor (CGM) or automated insulin delivery system (AID), ask if you can get this technology.
How can blood sugar management be measured or improved for people with diabetes and CKD when A1C is not reliable?
Unfortunately, there are no clear recommendations about blood sugar management in people with diabetes and CKD. Due to the limitations of A1C among those with CKD, some leaders in the field are encouraging people with CKD and diabetes and their healthcare teams to replace or supplement A1C with other measures of blood glucose management, such as CGM. CGM can help people monitor hypoglycemia, a particular risk as the kidneys fail and break down less insulin. Leaders are calling for more research on CGM and time in range as alternatives to A1C.
You can read more on the limitations of A1C here.
This article is part of a series on time in range.
The diaTribe Foundation, in concert with the Time in Range Coalition, is committed to helping people with diabetes and their caregivers understand time in range to maximize patients' health. Learn more about the Time in Range Coalition here.







